EarlyTox心毒性キット
EarlyTox 心毒性キットとは
心毒性化合物の同定を検討している研究者にとって、EarlyTox™心毒性キットは創薬の早い段階でより多くの化合物をスクリーニングすることを可能にします。これにより、リード化合物に優先順位を付け、より早く医薬品化学に取り組むことができるため、生産性が向上し、下流での広範な安全性試験に関連するコストを削減することができます。
EarlyTox 心毒性キットの特長
- 心毒性化合物を除去し、潜在的な薬剤候補を同定する。
- 384サンプルを数時間ではなく数分で測定
- 拍動特性に対する色素の非特異性影響を最小限に抑える。
- ウェル間のばらつきを低減し、データの質を向上
- 最大のシグナルダイナミックレンジ
- イソプロテレノール、ソタロール、プロプラノロールの3つの参照化合物に対するベンチマーク
EarlyTox™心毒性キットは、幹細胞由来の心筋細胞を用いた生体関連アッセイにおいて、心毒性化合物を同定するための迅速、簡便、かつ信頼性の高い蛍光ベースの方法を提供します。特許取得済みのマスキング技術と新規のカルシウム感受性インジケーターを活用することで、研究者は以下のことが可能になります:
EarlyTox心毒性キットのデータ
-
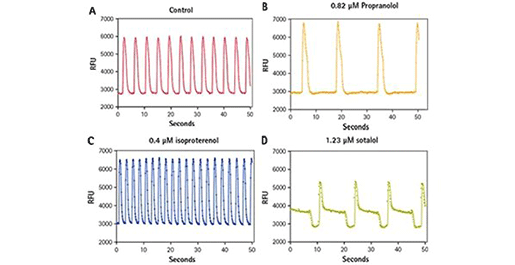
心筋細胞の拍動数に対する参照化合物の比較
(A) EarlyTox心毒性色素で2時間インキュベートした未処理のiPSC心筋細胞におけるカルシウムシグナルの変化をカルシウムピークで示す。(B)プロプラノロールはiPSC細胞におけるカルシウムのピーク頻度を遅くする。(C)イソプロテレノールはiPSC心筋細胞におけるカルシウムのピーク頻度を増加させる。(D)ソタロールはiPSC心筋細胞におけるカルシウムのピーク頻度を遅くし、正常パターンを変化させる。 -
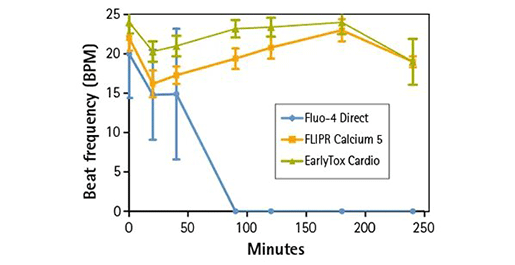
拍動周波数の比較
拍動頻度は4時間の間に記録された。すべてのウェルでEarlyTox心毒性染料の拍動頻度が最も高かった。 -
平均ピーク振幅に対する染料の影響
時間の経過とともに、EarlyTox心毒性色素の平均ピーク振幅が最も大きくなった。他の色素からのシグナルは時間とともに減少した。 -
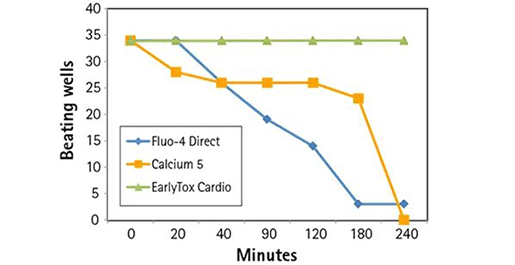
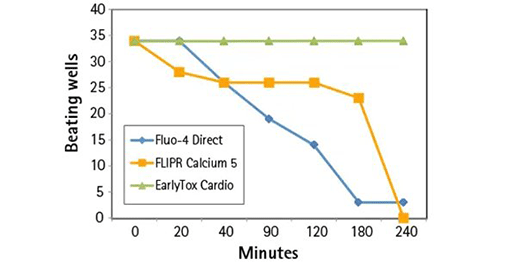
経時的な筋細胞拍動に対する色素の影響の比較
34個のコントロールウェルを4時間にわたって各染料で比較した。EarlyTox心毒性染料ウェルはすべて、4時間まで拍動を維持した。Fluo-4 DirectウェルおよびFLIPR Calcium 5 Kitウェルでは、沈黙したウェルがかなり早い段階で発生し、4時間後までにはほぼすべて消失した。
EarlyTox心毒性キットのテクノロジー
-
EarlyTox™ 心毒性キットは、化合物の毒性と有効性を予測するための均質なソリューションを提供します。
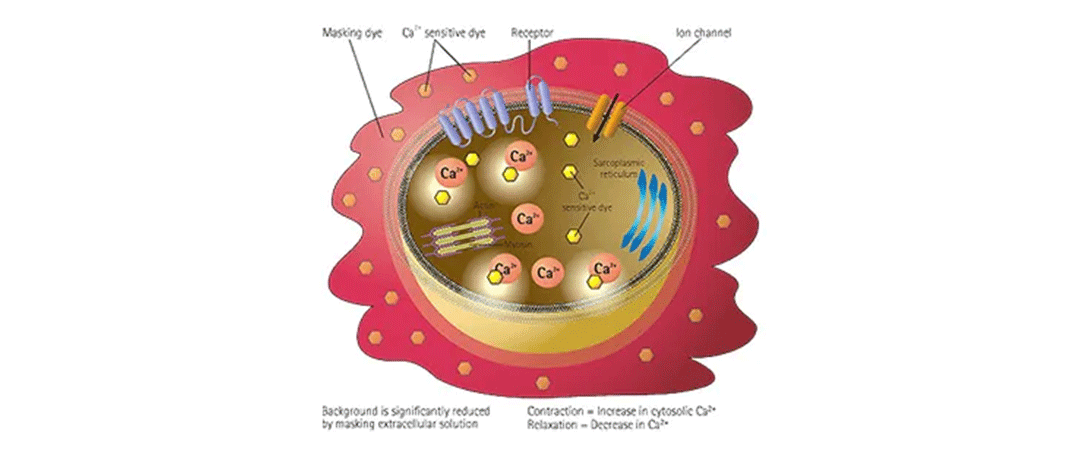
EarlyTox心毒性キットは、培養中に細胞質に吸収されるカルシウム感受性色素を利用します。色素が細胞質内のカルシウムイオンと結合すると蛍光強度が増加し、カルシウム濃度の変化を測定することができる。マスキング技術は細胞内には入らず、細胞外のバックグラウンド蛍光を減少させる。これにより、アッセイシグナルウィンドウが改善され、ビートパターンがより詳細に得られる。 -
心筋細胞の収縮-弛緩メカニズムにおけるカルシウムの役割
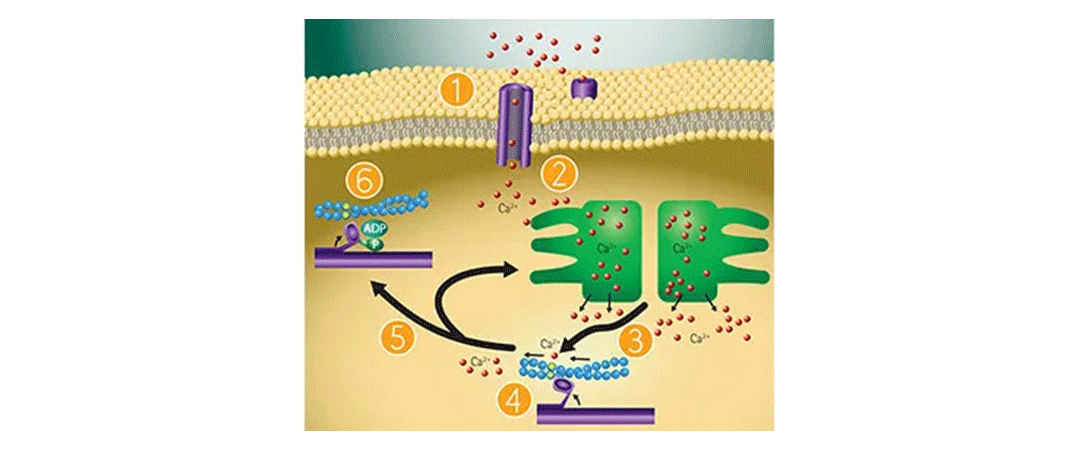
EarlyTox心毒性キットは、ピーク周波数(BPM)、ピーク振幅および拍動パターンに対する薬理学的化合物の影響を評価するために使用でき、幹細胞由来心筋細胞または初代心筋細胞で機能するように設計されています。ピーク周波数は、EarlyTox Cardiotoxicity Dyeによってモニターされた細胞内カルシウム濃度の変化から決定される。心筋細胞の収縮-弛緩におけるカルシウムの役割には以下のようなものがある: 2.1. 膜の脱分極が起こり、カルシウムチャネルが開き、カルシウムが細胞質に入る。2.2. 細胞内カルシウムが筋小胞体からのカルシウム放出を誘発する。2.3. 細胞質カルシウムがトロポニンに結合し、サルコメアを活性化する。2.4. 心筋細胞の収縮が起こる。2.5. 筋小胞体への能動輸送および細胞外液とのカルシウム交換によるカルシウムの除去。2.6. このサイクルが繰り返される。
EarlyTox心毒性キットに対応する製品・サービス
-
SpectraMax Paradigm マルチモードマイクロプレートリーダー

高速で設定可能なマイクロプレートリーダー1台でハイスループットスクリーニングが可能
-
SpectraMax iD3/iD5 マルチモードマイクロプレートリーダー
大型タッチスクリーンを備えた高感度マイクロプレートリーダー
-
FlexStation 3 マルチモードマイクロプレートリーダー

イオンチャネル・GPCR活性の測定に威力を発揮する
自動マルチチャンネルピペッター搭載マルチマイクロプレートリーダー -
SpectraMax i3x マルチモードマイクロプレートリーダー

研究ニーズに合わせて進化できるマイクロプレートリーダー
-
FLIPR Penta ハイスループットセルベーススクリーニングシステム

リード化合物の同定および化合物の安全性評価を目的とした
ハイスループットカイネティックスクリーニングに理想的なシステム